What is an AMA? Against medical advice is a phrase pertaining to a patient’s decision to discontinue therapy despite the advice of medical professionals.
Document… Document… Document!
Obtaining a defensible AMA:
Does the patient have the capacity to refuse care – are they capable of making a decision? Can the patient understand and communicate a rational decision? A&Ox4 is not good enough… You need to evaluate and describe the following:
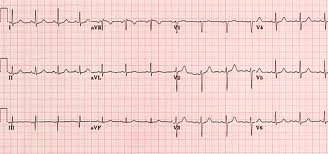
The primary purpose of obtaining a 12 lead ECG is to screen for cardiac ischemia. A normal 12 lead ECG does not mean that the patient is not having acute ischemia, injury or infarction! The patient may be in the early stages of the AMI and the infarction is evolving or the infarction has progressed passed the “acute phase”.
So, if you have educated your
patient, describing how a normal 12 lead ECG does not exclude them
from serious injury, permanent
disability and/or death,
evaluated their decision-making capacity and performed a patient
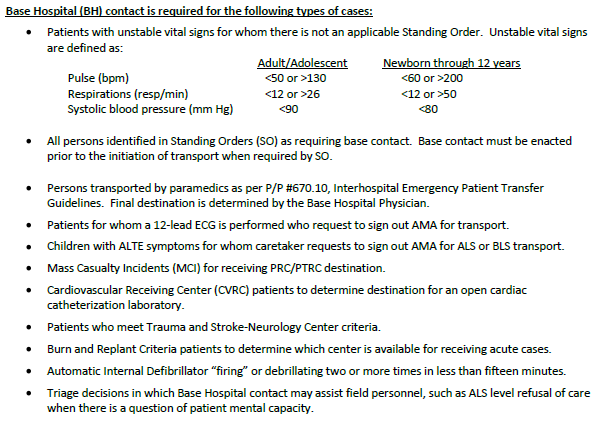
assessment – make base hospital contact and run the case by the
base hospital physician – do not assume the liability!! Remind the
patient of the benefits of transport!
“As in those patients presenting with ST-elevation MI, aspirin has been shown to provide significant benefit as secondary prevention among patients with unstable coronary syndromes (unstable angina/non-ST-elevation MI)” Circulation. 2011; 123:768-778
Don't forget the life-saving Aspirin!
SO-C-15 – Aspirin 324 mg PO given if none of the following exists:
Not taken in the last 4 hours
Pain radiates to mid-back or patient reports back pain
Taking an anticoagulant or antiplatelet
History of aspirin allergy
Recent history of asthma


The atypical clinical presentation of myocardial infarction increases with age and gender. Women and patients over the age of 55 can present with symptoms such as:
Neck, back, jaw and head pain
Syncope
Weakness
Sweating
Nausea
Dyspnea, shortness of breath or cough
In one study, 32 % of the AMI patients presented with atypical symptoms. Atypical symptoms were most prevalent in women over the age of sixty-five. The most common atypical symptoms reported by this group of patients were abdominal pain and dyspnea.
Lusiani, L., Perrone, A., Pesavento, R., Conte, G. Prevalence, clinical features, and acute course of atypical myocardial infarction. Angiology. 1994 Jan; 45(1):49-5
Risk factors for both typical and atypical AMI are:
Please remember the 12 lead ECG!!!!!
When administering Morphine intravenously, please be careful and push the Morphine slowly over 1-2 minutes. Do not push the Morphine in like a saline flush! It is sometimes easy in the heat of the moment and in our rush to help the patient, we go a little fast in pushing the Morphine IV...slow and easy will help the patient in the long run.
What happens when IV Morphine is pushed to fast?
2. Nausea and Vomiting
3. Syncope

